Glaucoma Surgery
For more information on the surgical treatments of glaucoma, jump to the relevant section below:
iStent Minimally Invasive Glaucoma Surgery
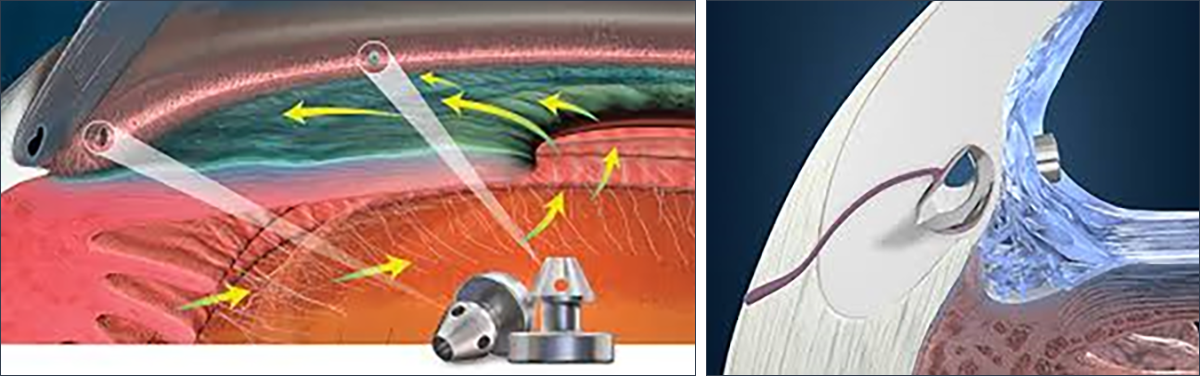
iStent surgery is a minimally invasive glaucoma surgery (MIGS) that involves implanting tiny titanium stents into the trabecular meshwork to improve fluid drainage and reduce intraocular pressure (IOP) in patients with mild-to-moderate open-angle glaucoma. It is typically performed in conjunction with cataract surgery, though it can be performed as a standalone procedure.
Procedure:
Pre-operatively: The nursing staff will offer you a relaxing medication (Diazepam) to help relieve any natural anxiety. Mr Leadbetter will come to see you and answer any questions you might have on the day. If combining iStent with cataract surgery, the nursing staff will dilate your eye by placing a tiny little tablet underneath your lower eyelid. This is the best way of dilating you pupil nicely for the operation.
In the operating theatre:
Anaesthetic: Mr Leadbetter performs the vast majority of iStent surgery with either topical and intracameral anaesthetic, or with a sub-tenon injection.
Topical anaesthesia involves numbing drops, and more numbing medicine into the front chamber of the eye at the very beginning of the surgery. You will not feel anything sharp or uncomfortable, though you will still be able to move the eye around, and feel pressure and cold.
A sub-tenon injection involves numbing drops, and then an injection of anaesthetic around the eye. There is a little more discomfort during the injection, but the eye will be nicely ‘frozen’ with this method. You won’t be able to move the eye, and the vision will be gone for several hours afterwards.
It is possible to be put to sleep for the operation with a general anaesthetic, though this is rarely necessary.
Procedure: You will generally be in the operating theatre for around 30 minutes for standalone surgery, and 60 minutes when combining with cataract surgery. We perform various safety checks before proceeding with the surgery. You will be laid down on a highly adjustable bed, and we will ensure you are completely comfortable before starting.
Your anaesthetic will then be given. If cataract surgery is being performed, this will be done first.
For the iStent procedure, you will have to tilt you head away from Mr Leadbetter, and hold this position for the procedure. A contact lens is placed onto the eye, the operating microscope is tilted, and the trabecular meshwork is brought into fine focus. Two iStents are then very carefully positioned into the trabecular meshwork to enhance fluid outflow. The iStent procedure normally takes 10-15 minutes. One eye will be done first, with the second eye at a later date if necessary.
Recovery: Patients go home the same day. Vision often improves within days, with full recovery in around 4 weeks. Anti-inflammatory drops are used for 4 weeks. The recovery following cataract surgery combined with iStent surgery is essentially identical to cataract surgery alone.
Indications:
- Mild-to-moderate open-angle, pseudoexfoliative, or pigmentary glaucoma.
- Patients needing IOP reduction or fewer glaucoma medications.
- Often combined with cataract surgery for those with both conditions.
Effectiveness:
- Reduces IOP by 20–44% (e.g., from ~23.5 mmHg to 13.8–14.6 mmHg) and medication use by 58–76% at 5–7 years.
- In clinical studies, 68% of patients with cataract surgery combined with iStent remained medication-free at 12 months with IOP ≤ 21 mmHg.
Risks:
- The procedure carries minimal risk. There is a very small risk of temporary corneal oedema, inflammation, or small bleeds (resolve within days to weeks).
- Rare: stent obstruction (4–6%), IOP increase, or vision reduction.
Further information:
https://glaucoma.uk/about-glaucoma/treatments-surgery/migs/
https://www.glaukos.com/en-uk/glaucoma/products/istent-inject-w/
Trabeculectomy with Mitomycin C:
Trabeculectomy augmented with Mitomycin C (MMC) is the gold standard surgical procedure used to treat glaucoma. It creates a new drainage pathway for fluid to leave the front chamber of the eye, lowering the intraocular pressure (IOP). MMC, an antimetabolite, is applied during surgery to enhance the procedure’s success by reducing scar tissue formation.
Procedure:
Pre-operatively: The nursing staff will offer you a relaxing medication (Diazepam) to help relieve any natural anxiety. Mr Leadbetter will come to see you and answer any questions you might have on the day.
In the operating theatre:
Anaesthetic: Mr Leadbetter performs the vast majority of trabeculectomy surgery with a sub-tenon injection. This involves numbing drops, and then an injection of anaesthetic around the eye. There is a little discomfort during the injection, but the eye will be nicely ‘frozen’ with this method. You won’t be able to move the eye, and the vision will be gone for several hours afterwards.
It is possible to be put to sleep for the operation with a general anaesthetic, though this is rarely necessary.
Procedure:
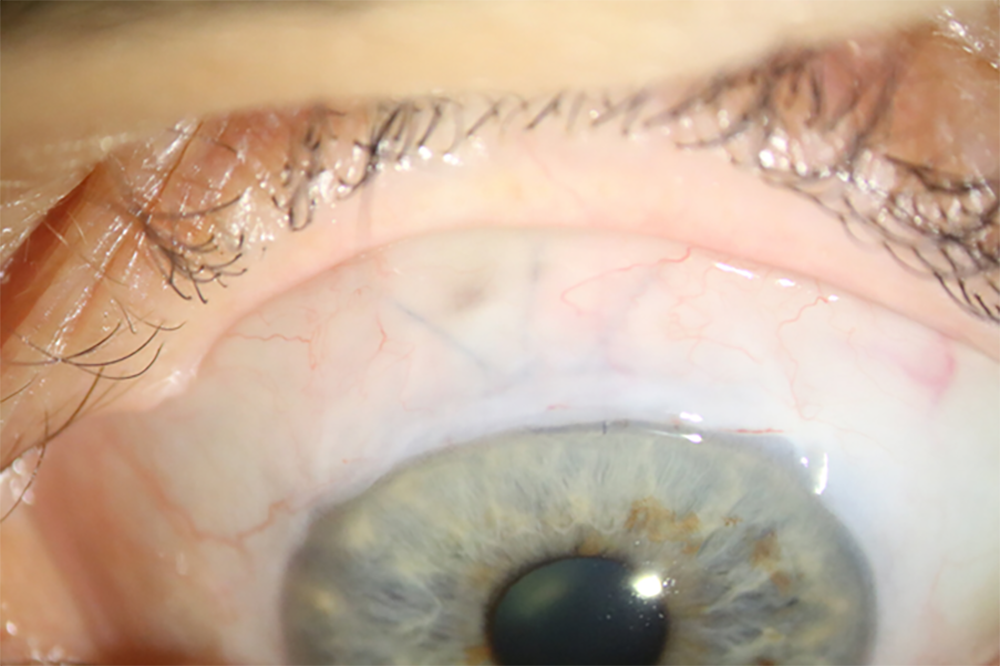
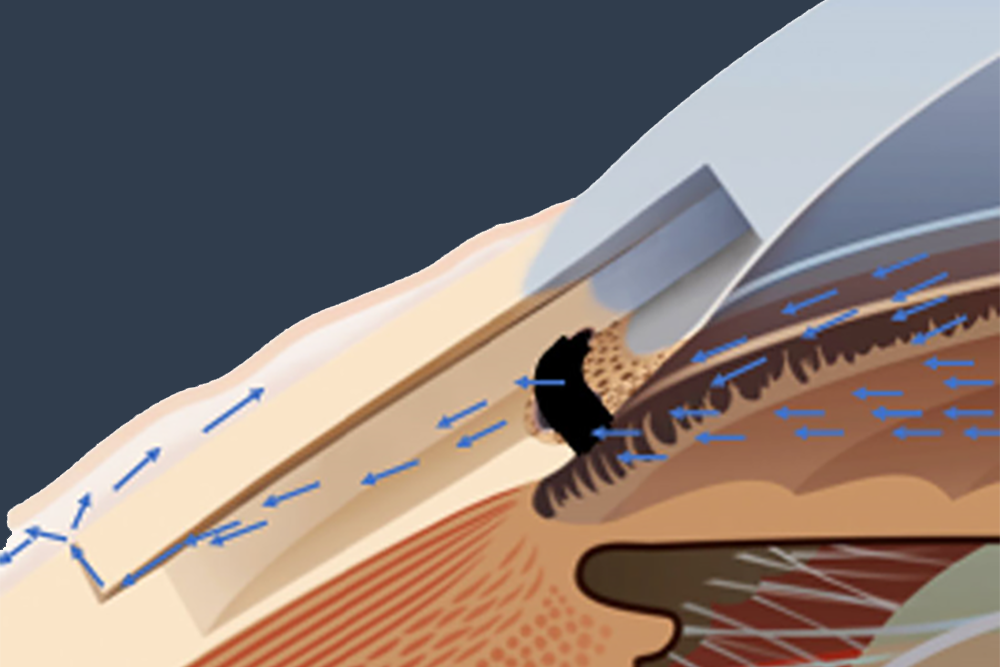
- Surgical Technique: A small flap is created in the tough white coat of the eye, with a hole at the base connecting to the front chamber. This allows fluid to exit the front chamber, forming a fluid filled ‘bleb’ under the skin covering the eye. This bypasses the usual drainage system, lowering the IOP.
- Mitomycin C Application: MMC is applied intraoperatively (for 3 minutes) to the scleral and conjunctival tissues to prevent scarring.
- Duration: The surgery takes about an hour.
Benefits:
- Significant IOP Reduction: Trabeculectomy with MMC can powerfully lower the IOP, with an average level of pressure of around 12mmHg following the operation.
- Long-Term Control: All glaucoma drops can be stopped on the day of trabeculectomy surgery in the operated eye. When the surgery is successful, most people will remain off glaucoma medications but occasionally drops will need to restart to help control the pressure.
- Effective for Advanced Cases: Particularly beneficial for patients with uncontrolled glaucoma or those unresponsive to less invasive treatments.
Risks:
- Complications: Risks include major bleeding or infection (around 1 %), low IOP, cataract formation, further surgery or vision loss.
- Around 1 in 5 patients will need a needling procedure, to break up scar tissue that has formed and inject further anti-scarring MMC. This is a quick procedure, usually under topical anaesthesia,
Postoperative Care:
- Wear an eye shield for the first few hours after surgery, and overnight for 1 week.
- Steroid drops are given 6 times a day for 6 weeks, and antibiotics 4 times a day for 4 weeks.
- It is important to avoid bending over, heavy lifting or strenuous activity for 4 weeks.
- The vision is likely to be blurry afterwards for several weeks and slowly recovers over 2 months. The spectacle prescription may change, so it is good to check this with your optician when Mr Leadbetter recommends this.
- Intensive follow-up is required to monitor IOP, bleb function, and potential complications, often involving suture adjustments or additional interventions. As a minimum, you will need to see Mr Leadbetter on day 1, week 1, week 3 and week 7 following the surgery. Occasionally further visits are required.
Outcomes:
- Studies show trabeculectomy with MMC achieves long-term IOP control in around 70% of patients, with many maintaining target IOP for years. However, success varies according to patient factors (e.g., age, glaucoma type). Regular monitoring is essential to manage complications and ensure bleb patency.
Trabeculectomy augmented with MMC is a highly effective procedure for managing severe or refractory glaucoma, offering significant IOP reduction but requiring careful postoperative management to optimise outcomes and minimise risks.
Further information:
https://glaucoma.uk/about-glaucoma/treatments-surgery/trabeculectomy-surgery/
Trabeculectomy bleb needling with Mitomycin C
Trabeculectomy bleb needling is a quick procedure used to restore the function of a failed or failing bleb after previous trabeculectomy surgery. The primary cause of failure is scar tissue formation that blocks the flow of aqueous humour from the eye, leading to elevated intraocular pressure (IOP).
Procedure:
- Purpose: To break down scar tissue around the original surgical site and re-establish proper fluid drainage to lower IOP and prevent further vision loss from glaucoma.
- Anaesthesia: It is typically performed using topical anaesthetic, with extra subconjunctival anaesthesia as necessary.
- Technique: A fine needle is inserted into the subconjunctival space (under the clear covering of the eye) near the bleb. Mr Leadbetter then uses sweeping motions to physically break apart the scar tissue and adhesions, which allows the trapped fluid to drain into the bleb reservoir. Once function has been restored, Mitomycin C (MMC) is injected to prevent new scar tissue from forming and to improve long-term success rates.
Post-Procedure Care:
- The eye will be covered with a shield, which is to be worn for the first few hours after surgery, and overnight for 1 week.
- You will be given steroid eye drops to be taken 6 times a day for 6 weeks, and antibiotic drops 4 times a day for 1 week.
- It is important to avoid bending over, heavy lifting or strenuous activity for 1 week.
- The vision is often a little blurry following the procedure, but recovers quickly.
Outcomes:
- Effectiveness: The procedure is often successful, with studies reporting success rates in restoring and improving drainage in over half of the cases. It is most effective when performed shortly after the original trabeculectomy operation fails.
- Risks: While generally considered safe, potential complications include bleeding inside the eye (hyphaema), infection, temporary low eye pressure (hypotony), or bleb leakage. If it doesn’ work, further surgery will be required.
Discussion with Duncan is important to answer any questions that you may have. For information about any additional conditions not featured within the site, please contact us for more information.






